January 19, 2011. New Jersey, USA
Yes, this case was a mystery that would not be solved or completed until research
pathologist in diagnostic medical mycology J
Dumanov (Mycological Institute sCRG EU US) was contacted and performed histopathology on the necrotized
sinus tissue and identified the Aspergillus fumigatus in vivo. Later
genomic methods specified sequences as A. terreus. For a detailed case
review see it as it was presented in detail by Gray and Dumanov at the
international conference Aspergillosis 4th in Rome February 2010.
Dumanov is a medical mycologist, toxicologist and research pathologist in
diagnostic medical mycology currently in the U.S. was interviewed by
IEHN to comment on his role in the case presented in the premier
episode of the Oprah Winfrey Network's Mystery Diagnosis series entitled "Fight to the Last Breath" broadcast January 5th and 19th, 2011.
We understand that you were involved in the early diagnostic stages of this case:
Yes, I was contacted in January 2005 while in the EU doing research study by Thomas Jones the husband of Liana Jones of the case presented in this Mystery Diagnosis premiere episode to review Liana's case. At the time I was very active in work associated with the Aspergilli and the coincidence with the Jones' case an my work as medical mycologist proved to be pivotal for the Jones' and quite interesting and involved at many levels over the next 6 years.
What interested you in this case?
The
short story is that is is about advancing medical mycology research, helping people and
saving lives. When Mr. Jones contacted me he wanted to know what else
may be involved with Liana's disease. I was reluctant to take on their
case initially feeling that there was nothing interesting here that was
not already covered her doctors. At the time Tom Jones, a
microbiologist and not a mycologist was very involved in the care and treatment of his wife
Liana. He noted there were more structures in the original pathology slides but his claims were disregarded by the labs and as this show depicts he was looking for all the answers to what
seemed to be a very grim prognosis. After returning and over a few
weeks of review and discussion I was convinced there were some valid
pathology questions raised and unanswered and that I could be of help
and at that point there was just no other answer given the specific
needs of the Jones' and the medical questions posed since there are
only a handful of researchers immediately available for their needs.
For a clinical research scientist as myself this case was about the etiology and
pathology of her disease both focal areas of my research work as a medical mycologist therefore
the case was accepted for scientific purposes and for that purpose it was satisfied with our invitation for the Rome medical presentation.
What were your histopathology findings?
I reviewed the original pathology slides and prepared other samples of newly submitted sinus tissue. My lab study was completed and report submitted on November 25,2006 of numerous biopsied and additional necrotized tissue samples from Liana's sinus and over many hours identified the presence of fungal mold in hyphal state along with many other structures associated with Aspergillus fumigatus. Follow up pathology by Maluf (June 2008) and genomics from University of Pennsylvania confirmed my findings. The difficulties in identification of invasive fungal mold are many many many and not easily performed. Every biological entity has a different form and this is more true for mold fungi due to their dimorphic / pleomorphic nature. It becomes even more complicated with the fact when fungi become clinically relevant when they invade animals - humans they become obscured by the tissue they invade. Even sample preparation poses a toxic risk and exposure to potentially infectious fungi. The study is very challenging and time consuming and a full cognition of fungal morphology in many states is required for identifying these pathogens. Even today mastery of this research commands a medical academic matrix rarely obtained by but a few medical scientists outside of research academics. In general almost all medical labs fail in identifying such pathogens. Identification
was challenging but concluded that the fungal mold was from the genus
Aspergillus and based on morphology and in situ presentation as
fumigatus, genomics later performed nominally added to specificity.
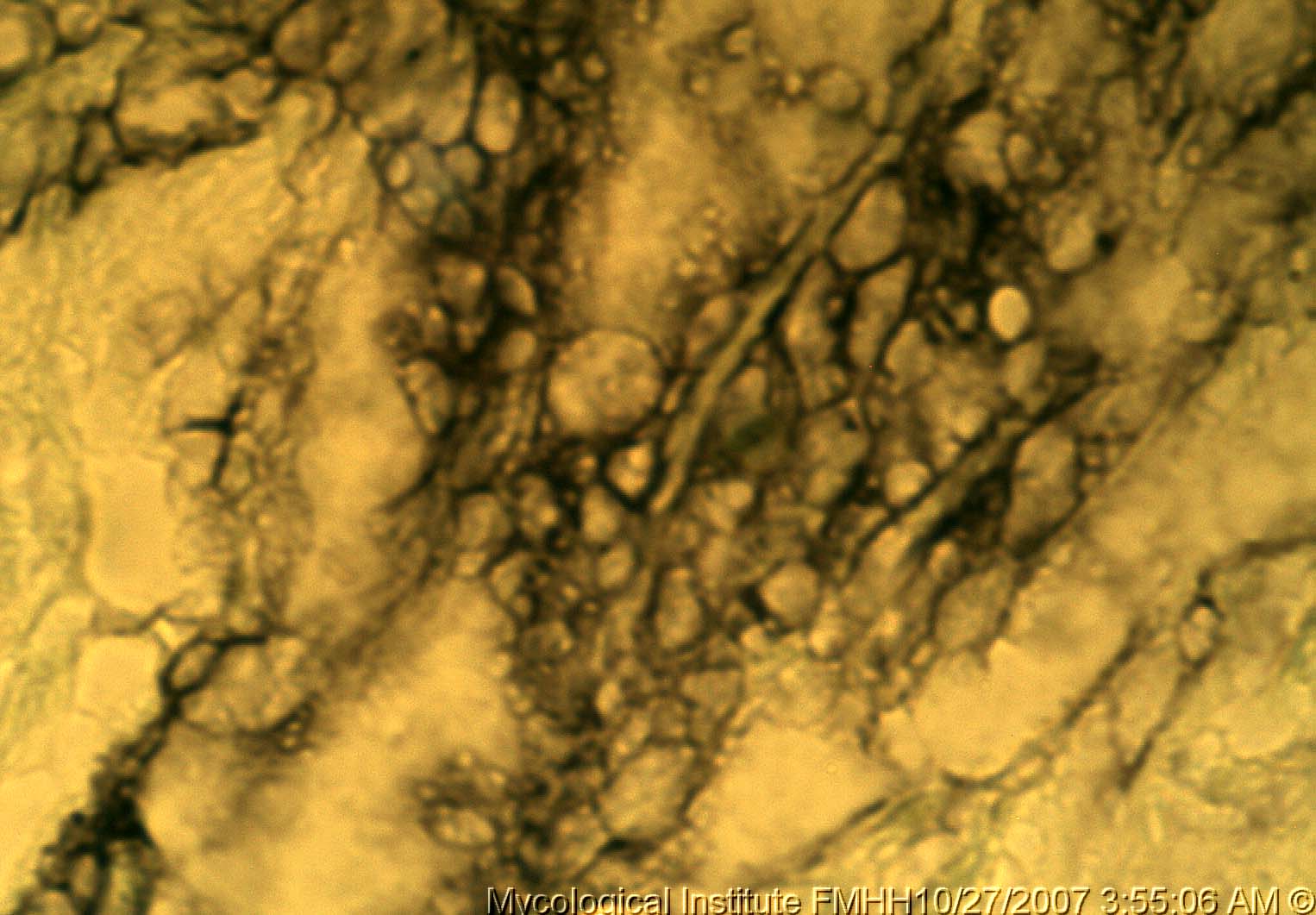 |
Jones' sinus - Invasive A. terreus. |
What affect did your findings have on the outcome of the case?
Having spent over a 100 hours on this case at every level. I
have never met either of the Jones but have met and worked with the
doctors involved in her diagnosis and treatment. Up to the time of my
involvement although mold fungi was suspect none were qualified or able to identify
any such presence in the tissue. My identification redirected the
diagnostic with added attention of my findings and ultimately the
genomics proved to be conclusive as Aspergillus terreus not previously
possible to be so discernible in vivo.
In
the final analysis rare cases such as this highlight that mold fungi
need to be considered in all out of the ordinary or inconclusive
diagnosis. Acute fungal sinusitis is normally treated effectively
within 4 weeks. Symptoms lasting longer in the immunocompetent are
considered chronic and may be indicative of invasive disease..
Under what circumstance should emphasis be placed for suspecting mold fungi as part of a diagnosis?
In general medical doctors and labs get it right given the old school. The new school tells us what we know now is that fungi play larger roles in a wide range of disease. Allergies, respiratory diseases including cystic fibrosis, bronchiectasis, atelectasis and nearly all cancers from neoplasia to necrosis involve may mold and yeast fungi. For anyone that has a cancer I do recommend the study of the pioneering work of Dr. Tullio Simoncini, MD Oncologist and see his published work "Cancer is a Fungus" and his many videos on the web. Many fungal related cancers may be cured when diagnosed early.
Do you accept patient cases like this on an ongoing basis?
Generally no. Travel, research, teaching and study load is exhausting and very busy but from time to time we accept cases of interest for patients, study and research publication. Cases may be submitted to us for consideration. Medical history is required, pathology, diagnosis, treating physician, clinic etc must be included: (type in-not a link)

Are there fees for research?
No, all of the research work of the subClinical Research Group (sCRG)
foundation in the US, UK and EU if accepted are at no cost. All related research and work
product is the confidential property of the sCRG with full privacy
guards of research subjects. If you need any special medical testing
that will be performed under direction of your own medical doctor or
their referral to specialists under your own medical coverage
provisions.
What other research are you and your group currently involved in at this time?
Current focus is the role of mycotoxins in immunotoxicology and the autoimmune disease conditions. There are
many of our related publications on the web that are available for
those with a clinical interest in diseases involving mold and other forms of fungi.
Thank you for your time.
Dumanov has made numerous appearances, medical publications and
presentations in the US and EU over the years and also appeared on the
Discovery Health Channel show "Is Your House Out to get You?" |